
A character-based digital intervention has been created for use by families and schools. It aims to support children’s emotional resilience and support healthy dialogue
Abstract
A collaborative project created a character-based digital programme to support early years emotional wellbeing. The programme includes accompanying materials for parents and schools to facilitate discussion and support systemic change. Early outcomes suggest it offers an effective means to support preschool children’s ability to recognise and discuss emotions, and there are plans to continue to develop and roll out the project.
Citation: Selby E, Allabyrne C (2021) Creating a digital programme to support children’s emotional wellbeing. Nursing Times [online]; 117: 1, 22-24.
Authors: Emma Selby is clinical nurse specialist and digital lead for Digital Mentality; Clare Allabyrne is associate professor at London South Bank University.
- This article has been double-blind peer reviewed
- Scroll down to read the article or download a print-friendly PDF here (if the PDF fails to fully download please try again using a different browser)
Introduction
Risk to an individual’s mental health begins in utero and continues throughout their lifespan (Pearson et al, 2013). It can be particularly heightened at times of developmental change, including the transition from infant to preschool, preschool to school-age child, child to adult, and working-age adult to retiree.
Having a negative experience during the perinatal period (from conception to one year old) can have a long-lasting impact on psychological wellbeing, affecting both physical and cognitive development into adulthood (McDaid et al, 2019). This provides a strong case for investing in promoting positive mental wellbeing in the early years to reduce the risk of lifelong mental health problems and their impact on an individual, generational and societal level. Early intervention is considered key for the development of resilience and coping strategies in later life. However, there remains a limited number of evidence-based platforms that can scale to universal use outside of specialist services, such as social care or children and young people’s mental health services (CYPMHS).
Literature review
The number of children and young people experiencing significant levels of mental distress continues to increase. In England in 2017, 13% of 5-19-year-olds had at least one mental disorder when assessed and 66% had contact with a professional service because of worries about mental health (NHS Digital, 2018). Within primary healthcare settings, GPs are seeing an increased number of preschool-age children with emotional and conduct disorders (Mughal and England, 2016). STEM4’s (2016) report highlighted that, over the previous five years, 78% of GPs had seen an increase in the number of young people with mental health problems and 61% had seen a rise in self-harm among young patients.
Khan (2016) identified an increasing demand for specialist children’s mental health services in the West, and the UK is no exception. A lack of mental health support for children at an early intervention stage escalates the demand for tier 3 services (for children at high risk). Behavioural concerns are the most common reasons for a CYPMHS referral, with a higher prevalence in hard-to-engage groups including looked-after children and low socioeconomic communities (House of Commons Education Committee, 2016). Conduct problems in early and middle childhood are associated with increased risks of mental health problems during late adolescence (National Collaborating Centre for Mental Health, 2013). This is supported by Broidy et al (2003), who found that 60% of people who had a conduct disorder (broad term for behavioural difficulties) at three years of age continued to exhibit challenging behaviour in adolescence, including substance misuse and criminality – and significant mental health problems.
National Institute for Health and Care Excellence (2013) guidance recommends social learning theory-based programmes as a first-line treatment in children’s emotional wellbeing. O’Connor et al (2012) showed the success of these interventions was higher with younger children, suggesting that early years intervention is essential.
Early years interventions usually work with parents and children together. There are a number of well-known parenting programmes that offer support and coaching to parents, including encouraging them to think about their children’s emotional wellbeing – the best known are the Incredible Years (Webster-Stratton et al, 2004) and the Triple P parenting programme (Sanders, 1999). However, the majority are group-based programmes that require parents to allocate an hour a week for 12 weeks. These typically run during the day, so exclude working parents (Khan et al, 2015) and many are run by CYPMHS, meaning many families do not meet the threshold for support and, therefore, do not benefit from this level of expertise.
Lindsay et al (2011) conducted a scoping study into the effectiveness of group parenting interventions when rolled out to the community. Although they provided evidence of the programmes’ efficacy, they found a number of barriers to engagement and sustainability. An average group size was 10 parents and they were predominantly mothers, highlighting that group capacity and equal access remained a problem. Of these participants, 25% left the programme before the end, which is a common difficulty in group-based parenting interventions. One of the main reasons for this was participants’ exposure to socioeconomic disadvantage and other adversities; however, parents also reported feelings of judgement or an implication they were bad parents for requiring the group. The study also found that differences in the leadership style and approach of the clinicians delivering the groups significantly affected the programmes’ uptake and impact when used at scale: the clinician’s skill and expertise had a significant impact on parents’ willingness to engage for the whole course. The study acknowledged and recommended that the use of parenting programmes alone would not be sufficient to improve children’s wellbeing and resilience.
A review of these interventions was included as part of Birmingham’s Brighter Future programme (Little et al, 2012). Randomised control trials were conducted to test the effect of three programmes designed to improve early years wellbeing, two of which were the Incredible Years and Triple P parenting programmes. The Incredible Years programme demonstrated good effect, but had high-cost implementation and high drop-out rates. Triple P showed no effect, which was partly because the trial involved slightly older children up to the age of nine, when difficult behaviours become more entrenched (Little et al, 2012).
In addition to the two parenting interventions, the third randomised control trial introduced the school programme Promoting Alternative Thinking Strategies (PATHS) to 56 schools (pathseducation.co.uk). PATHS is a programme for educators and counsellors that was designed to facilitate the development of self-control and emotional awareness through lesson plans. The programme showed some initial impact; however, due to the lack of systemic integration with home and parenting life, later follow-ups demonstrated little to no impact, strengthening the evidence for a systemic, social learning theory-based approach to supporting families (Little et al, 2012).
Cost implications
There is a cost associated with providing traditional interventions for behavioural difficulties. The average cost of a referral to a community CYPMHS is £2,338. NHS England (2016) estimated that 270,000 referrals are made to CYPMHS across the UK per year – around a third of which are rejected because they do not meet the entry threshold – resulting in an estimated national referral cost of £631,260,000. The annual short-term cost to primary care services for supporting emerging mental wellbeing disorders in young children was estimated at £1.58bn, when demand was lower (Department of Health, 2013).
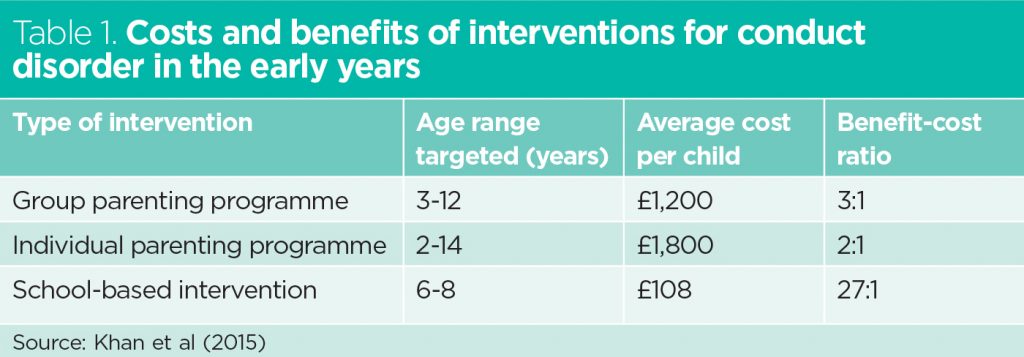
The Centre for Mental Health calculated the cost of delivering different types of interventions and their measurable benefits in terms of savings in future spending on health and other public services, and increases in future earnings (Khan et al, 2015). Table 1 the shows benefit-cost ratio of interventions for conduct disorder in the early years.
There is little evidence to be found on digital delivery of clinical intervention in relation to children’s emotional wellbeing. We, therefore, felt it was imperative to explore the possibility of emerging digital practices to provide access to existing knowledge bases in alternate and scalable ways.
“There is a cost associated with providing traditional interventions for behavioural difficulties”
Developing the project
Learning resources that help preschool-age children explore and enhance their emotional resilience are in an early stage of development. We therefore wanted to create an easily-accessed resource for emotional resilience training that could be used by a wide variety of professionals, who do not necessarily have specialist CYPMHS expertise, to provide a highly cost-effective primary intervention for improved emotional wellbeing.
A local collaboration was formed between clinical practitioners from CYPMHS, community facilitators from the Red Balloon Foundation (RBF) and Brickwall, and digital media specialists from Digital Mentality. The consortium used the NICE (2013) guideline for social learning theory-based interventions as a first-line treatment for behavioural difficulties, and previous clinical work in early years children’s emotional resilience and mental health literacy. The aim was to develop content that, if proved effective, could be converted into a programme that could be scaled digitally.
The consortium created a cartoon dragon called Embers, who formed the basis of a suite of media interventions for improved early years mental and emotional literacy that can be used by children, parents and teachers. The character was developed through co-design workshops with children and parents. A male character was selected to recognise the heightened need for young boys to reflect on a character exploring feelings. With multiple major characters featured throughout, a mixture of gender identities was used.
To provide a universally accessible platform, the consortium aimed to create Embers as a fully digital product with an animated series at the hub. Before seeking funding for this initiative, we required an early stage evaluation of the approach and programme content. The evaluation was to maximise our understanding of any ethical implications and the potential impact of this approach on preschool children’s emotional development. RBF created and hosted a pilot script and teachers’ content and we secured funding to produce a pilot episode, which was used as part of a wider MiLife Infants programme (milife.org.uk). The pilot episode focused on Embers exploring the different emotions experienced in different situations and how these make him feel and affect his behaviour towards others. Embers encourages children to learn words to describe their feelings and identify ways to make themselves feel better.
The pilot took place between June and November 2017 in schools across Epping, Essex. Over 2,000 primary school-age children in all year groups and 60 special educational needs (SEN) teachers watched the 30-minute animated Embers pilot. They were also able to use the associated lesson plans and teachers’ content. Parent information was provided through sessions held at school and worksheets sent home.
Of the participants, 21% were eligible for pupil premium for disadvantaged children, 16% received special educational needs support or had an education, health and care plan, and 13% spoke English as an additional language.
Results of the pilot phase
A Likert scale was used to evaluate the children’s learning following the programme, focusing on three key questions:
- Were they more likely to talk to a trusted adult about their emotional state after engaging with the platform?
- Did they learn something new about emotions through engagement with the story?
- Did they enjoy the story and associated platform content?
Field notes and project team discussions were also used to analyse the potential of the prototype digital package, and informal and formal feedback was gained from parents and SEN teachers. Focus groups were held with SEN teachers six and 12 months after the session to monitor its impact over time.
Feedback from children, teachers and parents
Sixty-nine per cent of the children who attended the session reported that they were more likely to talk to a trusted adult about their emotional state as a result of it. Eighty-nine per cent said they had learnt more about their emotions and 87% had enjoyed the story and associated content.
At the first focus group held with SEN teachers after six months, the teachers fed back that they continued to use the teacher content pack designed to accompany the programme. Two-thirds of teachers felt more confident in supporting their students’ emotional wellbeing because of the materials. During the second focus group, 12 months after the session, 72% of teachers said they continued to use the ‘emotion potion’ tool learnt as part of the programme; however, 87% felt the programme needed to be repeated to maintain its impact. When asked whether an animated development of the programme would be of benefit, 94% of attendees said it would be an “excellent” resource for young people, schools and families.
The purpose of this project was to establish engagement with the programme content from children and teachers, so parents were not formally surveyed as part of the study. However, anecdotal feedback from parents revealed strong positivity for a digital programme and a desire to have their own accompanying electronic resources that are easier to access than in-school parent-teacher sessions. We incorporated this feedback as we developed the project for the next research and funding round.
“We found that taking a digital approach to a core area of our job has allowed us to meet the needs of more people”
Next steps
Following the success of the pilot, the consortium chose a design theme that formed the final programme design, focusing on the digital aspect that could be scaled nationally. We decided that the website homepage would consist of the story of Embers and his friends, who face daily emotional difficulties such as sadness, anger and disappointment; these were identified as typical emotions for a target age range of 3-7-year-olds by our codesign group. Accompanying the cartoons would be a parenting app, children’s games and a teachers’ pack to reinforce learnings taken from the cartoons.
To create this content, the consortium’s clinicians developed the key learning points and the creative experts from RBF and Brickwall developed engaging and interesting scripts. We consulted young children on character creation and stories and held advisory groups with teachers to elicit ideas. A talented young artist was referred to us by her special educational needs teacher and is now an integral part of the design team, creating characters and bringing the story to life. All of the project’s content is based on the principles of social learning theory (Bandura, 1977) and self-determination theory (Ryan and Deci, 2017).
We launched the new content after receiving funding from Innovate UK. This means school nurses and children’s nurses across the country can now recommend the Embers school-readiness programme free of charge, using the website’s video adventure to explore core development skills and the professionally developed resources as home practice and tasks for the families they work with. Since it launched at the end of August 2020, there have been 480,000 interactions with the content.
Following this, and after two-and-a-half years of development and planning, we were awarded an Invention for Innovation Connect grant by the National Institute for Health Research to build two further prototype episodes and associated teachers’ and parents’ content. These will focus on managing difficult emotions and building confidence, and are currently in production. Live testing has begun and the results were being collated at the time of publication; they will be used to evaluate the use of a digital early-years intervention and to inform the next stage of the project.
As a result of these developments, we have trademarked the Embers concept and registered the company. Our aim now is to continue to measure the project’s impact over time and extend the scheme into a wider, national intervention study.
Potential benefits and implications
The project needs to be tested further for its longer-term benefit in enabling children, parents and teachers to discuss and engage in conversations about mental health-related issues that have previously been considered difficult. The pilot testing phase showed a positive impact that we anticipate could be increased in the future, to improve life-enhancing skills aimed at positive mental health, such as emotional recognition, emotional regulation, self-awareness, empathy and relationship-enhancement strategies. Another potential impact of the project is to enhance family dialogue around emotions. It can provide a tool to increase capacity for emotional literacy, including the vocalisation of emotions, which is a necessary skill to be developed and taken into young adulthood.
Because the project addresses a key government priority to improve access to psychological interventions, there are also a number of potential secondary impacts. This includes reducing the number of children and young people engaging in high-risk behaviours, such as using unhealthy responses in difficult situations due to an inability to self-regulate and identify strong emotions. The programme may, therefore, be useful within CYPMHS as well as schools, and could be used as a prevention strategy. This has the potential to help reduce the resource burden in CYPMHS, schools and preschools, with consequent financial savings.
It may also be possible to widen participation by offering the learning package to parents, who themselves may be experiencing mental health problems, thus offering an alternative intervention strategy to further promote their own understanding of emotional resilience and the impact of their emotional expression on their children. This could support healthy dialogue and avoid high-expressed emotion, and ultimately prevent parents from being separated from their children due to their own emotional state; this line of study needs to be tested further.
Discussion and conclusion
Developing an easily-accessed resource for children’s emotional resilience training that can be used by diverse personnel can provide a highly cost-effective primary intervention to improve emotional wellbeing. Our creative collaboration across different disciplines has proven an effective approach to advancing digital technologies across social innovations; we believe this is an efficient and economically sound approach to tackling a global health issue.
As nurses, we often believe technological innovation is not within our roles or skill sets; however, we found that taking a digital approach to a core area of our job has allowed us to meet the needs of more people. We would love to hear nurses’ suggestions for areas of health promotion and child development that we could address in future episodes. You can contact us and view the Embers programme by visiting here
Key points
- Research shows a link between conduct issues in childhood and mental health problems in later life
- Early years interventions that work with parents or schools have measurable cost benefits for health and other public services
- A collaborative project developed a digital programme to improve children’s emotional resilience
- The programme’s cartoons and accompanying teachers’ and parents’ resources received positive feedback
- Children reported increased ability to discuss emotions and the project aims to expand to improve healthy family dialogue
Bandura A (1977) Social Learning Theory. Prentice Hall.
Broidy LM et al (2003) Developmental trajectories of childhood disruptive behaviors and adolescent delinquency: a six-site, cross-national study. Developmental Psychology; 39: 2, 222-245.
Department of Health (2013) Annual Report of the Chief Medical Officer 2012. DH.
House of Commons Education Committee (2016) Mental Health and Wellbeing of Looked-after Children. House of Commons.
Khan L (2016) Missed Opportunities: a review of recent evidence into children and young people’s mental health. Centre for Mental Health.
Khan L et al (2015) Investing in Children’s Mental Health: a review of evidence on the costs and benefits of increased service provision. Centre for Mental Health.
Lindsay G et al (2011) Evaluation of the Parenting Early Intervention Programme. Department for Education.
Little M et al (2012) The impact of three evidence-based programmed delivered in public systems in Birmingham, UK. International Journal of Conflict and Violence; 6: 2, 260-272.
McDaid D et al (2019) The economic case for the prevention of mental illness. Annual Review of Public Health; 40, 373-389.
Mughal F, England E (2016) The mental health of young people: the view from primary care. Br J Gen Pract; 66: 651, 502-503.
National Collaborating Centre for Mental Health (2013) Antisocial Behaviour and Conduct Disorders in Children and Young People. NICE.
National Institute for Health and Care Excellence (2013) Antisocial Behaviour and Conduct Disorders in Children and Young People: Recognition, intervention and management. NICE.
NHS Digital (2018) Mental Health of Children and Young People in England, 2017. NHS Digital.
NHS England (2016) Children and Young People’s Mental Health Services Baselining Report. NHSE.
O’Connor TG et al (2012) Social learning theory parenting intervention promotes attachment-based caregiving in young children: randomized clinical trial. Journal of Clinical Child and Adolescent Psychology, 42: 3, 358-370.
Pearson et al (2013) Maternal depression during pregnancy and the postnatal period: risks and possible mechanisms for offspring depression at age 18 years. JAMA Psychiatry; 70: 12, 1312–1319.
Ryan RM, Deci EL (2017) Self-determination Theory: Basic Psychological Needs in Motivation, Development and Wellness. Guilford Press.
Sanders M (1999) Triple P – Positive Parenting Program: towards an empirically validated multilevel parenting and family support strategy for prevention of behaviour and emotional problems in children. Clinical Child and Family Psychology Review; 2: 2, 71-90.
STEM4 (2016) A Time Bomb Waiting to Explode: a Survey of GPs’ Concerns about Mental Health Services for Children and Young People. STEM4.
Webster-Stratton C et al (2004) Treating children with early-onset conduct problems: intervention outcomes for parent, child, and teacher training. Journal of Clinical Child and Adolescent Psychology, 33: 1, 105-124.

{kind=link}