1. Introduction
Anaemia in pregnancy is a global nutritional problem associated with increased risks of maternal mortality [
1
- Daru J.
- Zamora J.
- Fernandez-Felix B.M.
- Vogel J.
- Oladapo O.T.
- Morisaki N.
- et al.
Risk of maternal mortality in women with severe anaemia during pregnancy and post-partum: a multilevel analysis.
], Caesarean section [
2
- Drukker L.
- Hants Y.
- Farkash R.
- Ruchlemer R.
- Samueloff A.
- Grisaru-Granovsky S.
Iron deficiency anemia at admission for labor and delivery is associated with an increased risk for Cesarean section and adverse maternal and neonatal outcomes.
], low birth weight (LBW), small-for-gestational age, preterm birth, and perinatal and neonatal mortality [
3
- Pasricha S.R.
- Colman K.
- Centeno-Tablante E.
- Garcia-Casal M.N.
- Pena-Rosas J.P.
Revisiting WHO haemoglobin thresholds to define anaemia in clinical medicine and public health.
,
4
- Rahman M.M.
- Abe S.K.
- Rahman M.S.
- Kanda M.
- Narita S.
- Bilano V.
- et al.
Maternal anemia and risk of adverse birth and health outcomes in low- and middle-income countries: systematic review and meta-analysis.
]. It is estimated that, in 2016, 40% of pregnant women (95% CI: 36.4 to 44.7%) had anaemia globally, with the highest prevalence in the WHO regions of South-East Asia (58.2%) and the lowest in the Americas (25.5%) [
5
- Owen P.
- Donnet M.L.
- Ogston S.A.
- Christie A.D.
- Howie P.W.
- Patel N.B.
Standards for ultrasound fetal growth velocity.
]. As of 2020, prevalence of anaemia in women aged 15 to 49 years, by pregnancy status (percentage) is considered as an indicator to assess progress towards Sustainable Development Goal 2: End hunger, achieve food security and improved nutrition and promote sustainable agriculture by the United Nations Statistical Commission [
6
- Bertino E.
- Di Battista E.
- Bossi A.
- Pagliano M.
- Fabris C.
- Aicardi G.
- et al.
Fetal growth velocity: kinetic, clinical, and biological aspects.
] and reported in the World Health Statistics 2020 [
7
World Health Organization
World health statistics 2020: monitoring health for the SDGs, sustainable development goals.
]. Achieving a 50% reduction in anaemia among women 15–49 years of age is relevant to the UN Sustainable Development Goal [] and World Health Organization (WHO) global nutrition target for 2025 [
9
Using fractional polynomials to model curved regression relationships.
].
In 1958, a WHO Study Working Group on Iron Deficiency Anaemia met in Geneva, Switzerland and determined that, for adult pregnant women, haemoglobin (Hb) concentrations below 100 g/L were indicative of anaemia [
10
World Health Organization
Study group on iron deficiency A, world health O. Iron deficiency anaemia: report of a study group [meeting held in Geneva from 29 September to 4 October 1958].
]. This cut-off was based on the analysis of haematological data derived from studies of apparently normal populations and was intended for use in nutritional surveys in different parts of the world. In 1967, WHO defined maternal anaemia as an Hb concentration below 110 g/L at any gestational age [
11
WHO Scientific Group on Nutritional Anaemias & World Health Organization
Nutritional anaemias: report of a WHO scientific group [meeting held in Geneva from 13 to 17 March 1967].
]. Other thresholds were suggested by the US Centers for Disease Control and Prevention (CDC), expert clinical organisations, and individual clinical and research laboratories [
3
- Pasricha S.R.
- Colman K.
- Centeno-Tablante E.
- Garcia-Casal M.N.
- Pena-Rosas J.P.
Revisiting WHO haemoglobin thresholds to define anaemia in clinical medicine and public health.
,
12
- Muñoz M.
- Peña-Rosas J.P.
- Robinson S.
- Milman N.
- Holzgreve W.
- Breymann C.
- et al.
Patient blood management in obstetrics: management of anaemia and haematinic deficiencies in pregnancy and in the post-partum period: NATA consensus statement.
]. WHO currently recommends Hb cut-offs below which individual women should be defined as anaemic, by trimester of pregnancy (first trimester:
13
Recommendations to prevent and control iron deficiency in the United States. Centers for disease control and prevention. MMWR Recommendations and reports: Morbidity and mortality weekly report Recommendations and reports. 1998;47(Rr–3):1–29.
,
14
WHO
WHO recommendations on antenatal care for a positive pregnancy experience.
]. WHO also considers a normal Hb range in women by trimester as the assessment basis for blood transfusion, when needed [
15
World Health Organization
Blood transfusion safety T. The clinical use of blood: handbook.
].
The US CDC cut-offs were derived from gestational month-specific 5
th centile values for pooled Hb data from four small European studies (UK 1982,
n = 45; Sweden 1975,
n = 50; Finland 1980,
n = 32; Finland 1977,
n = 267) involving ‘healthy’ women [
16
- Puolakka J.
- Janne O.
- Pakarinen A.
- Jarvinen P.A.
- Vihko R.
Serum ferritin as a measure of iron stores during and after normal pregnancy with and without iron supplements.
,
17
- Taylor D.J.
- Mallen C.
- McDougall N.
- Lind T.
Effect of iron supplementation on serum ferritin levels during and after pregnancy.
,
18
- Sjostedt J.E.
- Manner P.
- Nummi S.
- Ekenved G.
Oral iron prophylaxis during pregnancy – a comparative study on different dosage regimens.
,
19
- Svanberg B.
- Arvidsson B.
- Norrby A.
- Rybo G.
- Solvell L.
Absorption of supplemental iron during pregnancy – a longitudinal study with repeated bone-marrow studies and absorption measurements.
]. The trimester-specific cut-offs were based on the mid-trimester values [
20
CDC criteria for anemia in children and childbearing-aged women. MMWR Morbidity and mortality weekly report. 1989;38(22):400–4.
]; cut-offs for the first trimester, when most women were initially seen for antenatal care, were based on a late-trimester value.
The need for better quality data to redefine the cut-offs in both pregnancy and childhood has been recognised for some time. In 2015, WHO initiated a project to review the Hb concentration cut-offs used to define anaemia in individuals and populations; review its social, biological, behavioural, environmental, and contextual determinants, and assess the expected impact of public health interventions for preventing and controlling anaemia and Hb concentrations [
21
- da Silva Lopes K.
- Takemoto Y.
- Garcia‐Casal M.N.
- Ota E.
Nutrition‐specific interventions for preventing and controlling anaemia throughout the life cycle: an overview of systematic reviews.
]. In 2018, experts, policymakers and programme implementers met to review key information and identify knowledge gaps relating to the diagnosis of anaemia [
22
- Garcia-Casal M.N.
- Pasricha S.R.
- Sharma A.J.
- Pena-Rosas J.P.
Use and interpretation of hemoglobin concentrations for assessing anemia status in individuals and populations: results from a WHO technical meeting.
]. The paucity of data relating maternal, newborn and child health outcomes to Hb values was also confirmed in a recent review, which stressed that not enough is known about the gestational age-specific Hb thresholds that predict health risk/protection for mother and infant [
23
- Young M.F.
- Oaks B.M.
- Tandon S.
- Martorell R.
- Dewey K.G.
- Wendt A.S.
Maternal hemoglobin concentrations across pregnancy and maternal and child health: a systematic review and meta-analysis.
].
To gather evidence to support updating recommendations for Hb concentrations during pregnancy that are associated with good maternal and child health outcomes, pooling high-quality individual-level data from prospective cohort studies was considered an imperative [
23
- Young M.F.
- Oaks B.M.
- Tandon S.
- Martorell R.
- Dewey K.G.
- Wendt A.S.
Maternal hemoglobin concentrations across pregnancy and maternal and child health: a systematic review and meta-analysis.
]. Thus, WHO searched for data sets that could provide the required populations, according to the characteristics identified previously for establishing international standards for human growth and development [
24
Rationale for developing a new international growth reference.
].
The Fetal Growth Longitudinal Study (FGLS), a major component of the INTERGROWTH-21
st Project [
25
- Villar J.
- Altman D.G.
- Purwar M.
- Noble J.A.
- Knight H.E.
- Ruyan P.
- et al.
The objectives, design and implementation of the INTERGROWTH-21st Project.
], was considered an appropriate source for such information because: a) populations were selected within defined geographical areas with absent or low levels of major, known, non-microbiological contamination, at an altitude of less than 1600 m; in addition, high educational level and socio-economic status, and low perinatal mortality rates, were present at population level; b) the women enrolled from these populations were healthy, educated and well-nourished; c) they had received quality-of-care pregnancy and delivery health services; d) their pregnancies were well-dated; e) they had very low rates of adverse maternal, perinatal and neonatal outcomes, and f) their children had satisfactory growth and neurodevelopment at 2 years of age [
25
- Villar J.
- Altman D.G.
- Purwar M.
- Noble J.A.
- Knight H.E.
- Ruyan P.
- et al.
The objectives, design and implementation of the INTERGROWTH-21st Project.
,
26
- Villar J.
- Fernandes M.
- Purwar M.
- Staines-Urias E.
- Di Nicola P.
- Cheikh Ismail L.
- et al.
Neurodevelopmental milestones and associated behaviours are similar among healthy children across diverse geographical locations.
,
27
- Villar J.
- Cheikh Ismail L.
- Staines Urias E.
- Giuliani F.
- Ohuma E.O.
- Victora C.G.
- et al.
The satisfactory growth and development at 2 years of age of the INTERGROWTH-21st Fetal Growth Standards cohort support its appropriateness for constructing international standards.
,
28
- Villar J.
- Papageorghiou A.T.
- Pang R.
- Ohuma E.O.
- Cheikh Ismail L.
- Barros F.C.
- et al.
The likeness of fetal growth and newborn size across non-isolated populations in the INTERGROWTH-21st Project: the fetal growth longitudinal study and newborn cross-sectional study.
,
29
- Papageorghiou A.T.
- Ohuma E.O.
- Altman D.G.
- Todros T.
- Cheikh Ismail L.
- Lambert A.
- et al.
International standards for fetal growth based on serial ultrasound measurements: the Fetal Growth Longitudinal Study of the INTERGROWTH-21st Project.
].
Hence, this paper provides, for the first time, normative Hb trajectories to establish gestational age-specific distributions that are compatible with functional health outcomes up to 2 years of age, as well as normal population thresholds for Hb in pregnancy. These parameters complement the international standards for early and late fetal growth, maternal weight gain, symphysis fundal height, and newborn size and body composition produced from the same FGLS data set [
29
- Papageorghiou A.T.
- Ohuma E.O.
- Altman D.G.
- Todros T.
- Cheikh Ismail L.
- Lambert A.
- et al.
International standards for fetal growth based on serial ultrasound measurements: the Fetal Growth Longitudinal Study of the INTERGROWTH-21st Project.
,
30
- Cheikh Ismail L.
- Bishop D.C.
- Pang R.
- Ohuma E.O.
- Kac G.
- Abrams B.
- et al.
Gestational weight gain standards based on women enrolled in the fetal growth longitudinal study of the INTERGROWTH-21st Project: a prospective longitudinal cohort study.
,
31
- Papageorghiou A.T.
- Ohuma E.O.
- Gravett M.G.
- Hirst J.
- da Silveira M.F.
- Lambert A.
- et al.
International standards for symphysis-fundal height based on serial measurements from the fetal growth longitudinal study of the INTERGROWTH-21st Project: prospective cohort study in eight countries.
,
32
- Papageorghiou A.T.
- Kennedy S.H.
- Salomon L.J.
- Ohuma E.O.
- Cheikh Ismail L.
- Barros F.C.
- et al.
International standards for early fetal size and pregnancy dating based on ultrasound measurement of crown-rump length in the first trimester of pregnancy.
,
33
- Villar J.
- Cheikh Ismail L.
- Victora C.G.
- Ohuma E.O.
- Bertino E.
- Altman D.G.
- et al.
International standards for newborn weight, length, and head circumference by gestational age and sex: the newborn cross-sectional study of the INTERGROWTH-21st project.
,
34
- Villar J.
- Puglia F.A.
- Fenton T.R.
- Cheikh Ismail L.
- Staines-Urias E.
- Giuliani F.
- et al.
Body composition at birth and its relationship with neonatal anthropometric ratios: the newborn body composition study of the INTERGROWTH-21st Project.
].
2. Methods
This work is reported following the STROBE guidelines [
35
- Ev Elm
- Altman D.G.
- Egger M.
- Pocock S.J.
- Gøtzsche P.C.
- Vandenbroucke J.P.
Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies.
].
2.1 Study design
A secondary analysis of prospective, population-based, longitudinal, observational cohort study from 2009 to 2016 to generate maternal haemoglobin normative centiles in uncomplicated pregnancies in women receiving optimal antenatal care. The INTERGROWTH-21
st Project consisted of several interrelated studies with the principal aim of evaluating growth, health, nutrition and development from less than 14 weeks’ gestation to 2 years of age, using the same conceptual framework as the WHO Multicentre Growth Reference Study (MGRS) [
36
- de Onis M.
- Garza C.
- Victora C.G.
- Onyango A.W.
- Frongillo E.A.
- Martines J.
The WHO multicentre growth reference study: planning, study design, and methodology.
].
2.2 Study site and population selection
2.2.1 Setting
The INTERGROWTH-21
st Project was carried out between 2009 and 2016 across eight diverse geographically delimited urban areas in: Pelotas (Brazil), Turin (Italy), Muscat (Oman), Oxford (UK), Seattle (USA), Beijing (China), Nagpur (India), and Nairobi (Kenya) [
25
- Villar J.
- Altman D.G.
- Purwar M.
- Noble J.A.
- Knight H.E.
- Ruyan P.
- et al.
The objectives, design and implementation of the INTERGROWTH-21st Project.
]. The selection criteria at the cluster level were: the areas had to be located at an altitude
2.2.2 Participants
The participants were selected based upon criteria for optimal health, nutrition, education and socioeconomic status, needed to construct international standards [
24
Rationale for developing a new international growth reference.
]. At each study site, we recruited women with no clinically relevant obstetric, gynaecological or medical history, who initiated antenatal care in early pregnancy i.e., +0 weeks’ gestation by menstrual dates, and met the entry criteria of optimal health, nutrition, education and socio-economic status. A detailed description of the entry criteria and definitions has been published previously [
25
- Villar J.
- Altman D.G.
- Purwar M.
- Noble J.A.
- Knight H.E.
- Ruyan P.
- et al.
The objectives, design and implementation of the INTERGROWTH-21st Project.
]. For example, adequate nutritional status was defined in the first trimester according to maternal height (≥153 cm), body mass index (BMI, ≥18.5 and 2), Hb level (≥110 g/L), and not receiving treatment for anaemia or following any special diets (e.g., vegetarian with no animal products). This resulted in a group of educated, affluent, clinically healthy women with adequate nutritional status, who by definition were at low risk of adverse maternal and perinatal outcomes.
The FGLS exclusion criteria included hypertension (defined as systolic ≥140 mmHg or diastolic ≥90 mmHg) in a past pregnancy or in the first trimester of the present pregnancy; chronic hypertension on treatment, and a past history of preeclampsia, eclampsia or Haemolysis Elevated Liver enzymes and Low Platelets (HELLP) syndrome. FGLS also excluded women if their pregnancies became complicated by criteria specified a
priori, including fetal death, congenital anomaly, severe or catastrophic medical morbidity not evident at enrolment (such as cancer or HIV), severe unanticipated conditions related to the pregnancy (such as severe preeclampsia or eclampsia), and those identified during the study who no longer fulfilled the entry criteria (e.g. women who started smoking during pregnancy or had an episode of malaria) [
25
- Villar J.
- Altman D.G.
- Purwar M.
- Noble J.A.
- Knight H.E.
- Ruyan P.
- et al.
The objectives, design and implementation of the INTERGROWTH-21st Project.
].
Gestational age was calculated from the date of the last menstrual period provided: the woman had a regular 24–32-day menstrual cycle, she had not been using hormonal contraception or breastfeeding in the preceding 2 months, and any discrepancy between the gestational ages based on last menstrual period and crown-rump length, measured by ultrasound between 9
+0 and 13
+6 weeks’ gestation, was 7 days or less. The dating scan was undertaken using standard study criteria for measuring crown-rump length [
37
- Ioannou C.
- Sarris I.
- Hoch L.
- Salomon L.
- Papageorghiou A.
Standardisation of crown-rump length measurement.
]. Dedicated research staff then performed an ultrasound scan every 5 weeks (± 1 week) until delivery to assess fetal growth. At each visit, information was collected about the pregnancy, as well as the results of blood tests (including Hb) taken as part of routine antenatal care that was provided separately to the study’s requirements. The gestational age at which those tests were taken varied depending on local protocols as this was a pragmatic study that aimed to mimic routine clinical practice in the different settings.
2.3 Haemoglobin analysis
The primary objective of this analysis of the FGLS data was two-fold: (a) to describe Hb ranges and trajectories in a population of optimally healthy women with good pregnancy, perinatal and neonatal outcomes, whose children had satisfactory postnatal growth and development up to 2 years of age so as to establish gestational age-specific distributions and populations thresholds for normal Hb in pregnancy, and (b) to define prevalence thresholds to diagnose adequate Hb concentrations in pregnancy at the individual level and the prevalence of anaemia at population level.
The Hb tests were taken as part of routine antenatal care, i.e., in relation to laboratory tests, 1) we relied on collecting the results of available routine blood tests; 2) the commercially available instruments for assessing Hb were not standardised across sites; and 3) information on the use of preventive or therapeutic iron and folic acid-containing supplements or calcium supplements, was collected from medical records. Although the eight study sites were not asked to follow a specific protocol, we have documented carefully the biochemical methods of Hb determination they used. All sites assessed Hb concentration from venous blood samples using commercially available methods (automatised colorimetry, automatised turbidimetry, high efficiency liquid chromatography, sysmex autoanalyser, automated flow fluorescent analyser, photometric method using automated cell counter, high-efficiency liquid chromatography and cyanide-free sodium lauryl sulphate) of Hb assessment that are widely used in routine patient care and considered highly reliable [
38
- Whitehead Jr., R.D.
- Mei Z.
- Mapango C.
- Jefferds M.E.D.
Methods and analyzers for hemoglobin measurement in clinical laboratories and field settings.
].
2.4 Statistical methodology
Our overall aim was to produce Hb centiles that change smoothly with gestational age and maximise simplicity without compromising model fit. We followed the same statistical methodology and approach previously described [
39
Statistical methodology for constructing gestational age-related charts using cross-sectional and longitudinal data: the INTERGROWTH-21st Project as a case study.
,
40
Statistical considerations for the development of prescriptive fetal and newborn growth standards in the INTERGROWTH-21st project.
] for the analyses of already published international standards [
29
- Papageorghiou A.T.
- Ohuma E.O.
- Altman D.G.
- Todros T.
- Cheikh Ismail L.
- Lambert A.
- et al.
International standards for fetal growth based on serial ultrasound measurements: the Fetal Growth Longitudinal Study of the INTERGROWTH-21st Project.
,
30
- Cheikh Ismail L.
- Bishop D.C.
- Pang R.
- Ohuma E.O.
- Kac G.
- Abrams B.
- et al.
Gestational weight gain standards based on women enrolled in the fetal growth longitudinal study of the INTERGROWTH-21st Project: a prospective longitudinal cohort study.
,
33
- Villar J.
- Cheikh Ismail L.
- Victora C.G.
- Ohuma E.O.
- Bertino E.
- Altman D.G.
- et al.
International standards for newborn weight, length, and head circumference by gestational age and sex: the newborn cross-sectional study of the INTERGROWTH-21st project.
,
41
- Villar J.
- Giuliani F.
- Bhutta Z.A.
- Bertino E.
- Ohuma E.O.
- Ismail L.C.
- et al.
Postnatal growth standards for preterm infants: the Preterm Postnatal Follow-up Study of the INTERGROWTH-21st Project.
].
The first step was to assess the variation in maternal Hb across different study sites to determine whether we could pool the data to estimate international normative values. The criteria used to judge similarities among study sites was based on WHO recommendations for analysing human growth data [
42
Group WMGRS
Assessment of differences in linear growth among populations in the WHO multicentre growth reference study.
]. In brief, we first inspected the data visually comparing patterns across sites. We then applied variance component analysis (analysis of variance (ANOVA)) to calculate the percentage of variance in the longitudinal maternal Hb concentrations from variance between sites and the estimated variance in individuals within a site (within-site variance). We treated gestational age as a fixed effect, whereas sites and individuals were treated as random effects in a multi-level linear regression model.
Having satisfied the criteria for pooling, we used the pooled data to construct smoothed centiles of maternal Hb according to gestational age using fractional polynomial regression that models the mean and standard deviation (SD) separately as a smooth function of gestational age. The best fitting powers for the mean and SD of maternal Hb according to gestational age were provided by the second and first-degree fractional polynomials, respectively. Goodness of fit of the resultant models was assessed as previously described for the INTERGROWTH-21
st data by Ohuma and Altman [
39
Statistical methodology for constructing gestational age-related charts using cross-sectional and longitudinal data: the INTERGROWTH-21st Project as a case study.
], i.e., visual inspection of the overall model fit by comparing empirical centiles (calculated per completed week of gestation, e.g. 38 weeks = 38+0 – 38+6 weeks’ gestation) to the fitted centiles, a plot of the residuals (observed values minus fitted values) according to gestational age, a quantile-quantile (Q‐Q) plots of the residuals to assess normality, and a plot of fitted z-scores across gestational ages.
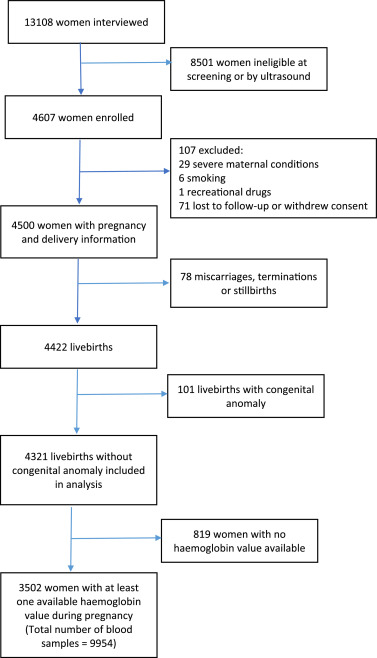
We then conducted various sensitivity analyses: 1) comparing the fitted smoothed centiles of longitudinal Hb data (n = 3502 women, 9954 observations) to a cross-sectional random sample of Hb data between 14+0 and 40+0 weeks’ gestation for each woman included in the study (n = 3502 observations) to evaluate whether multiple Hb values per women resulted in reduced error variance and consequently reduced variance of the estimated centiles; 2) comparing the total pooled sample (n = 3502 women) with the sample (n = 3364 women) that excluded those mothers who delivered preterm, i.e. less than 37 weeks’ gestation (n = 138 women), and then superimposing the two sets of fitted centiles to evaluate whether there were differences in maternal Hb among women delivering preterm compared to term newborns; and 3) excluding each site’s Hb data one at a time, refitting the centiles (seven sites’ data), and comparing the fitted (i.e., 3rd, 50th and 97th centiles) on the basis of fractional polynomial regression between the pooled data (eight sites) and the reduced datasets (one site excluded at a time) to establish whether there was any site-specific influence to the derived smoothed pooled maternal Hb centiles.
Descriptive analyses were used to summarise data on supplementation information that was available and collected as part of routine care. The supplementation was provided as prophylaxis as applied in routine practice following country-specific guidelines. In addition, for each site, we calculated empirical Hb centiles (specifically, 3rd, 5th, 10th, 50th, 90th, 95th and 97th centiles) and then computed the median across all eight sites to obtain Hb centiles for situations where gestational age is unknown. All analyses were performed in STATA, version 15, software (StataCorp LP, College Station, TX, USA).
The next step was to decide the approach for establishing thresholds for Hb concentration to define anaemia at individual level. Such thresholds are applied to judge the location of a single value in relation to the median of the normative distribution, i.e. to assess an individual’s status.
The definition of “normality” is conventionally set at 2 SD below (or above) a standard or normative median, but this is frequently rounded up to the 3
rd (or 97
th) centile in most international guidelines and literature [
43
- de Onis M.
- Borghi E.
- Arimond M.
- Webb P.
- Croft T.
- Saha K.
- et al.
Prevalence thresholds for wasting, overweight and stunting in children under 5 years.
]. We used this value to define the most severe threshold of Hb concentration in this population of healthy pregnant women.
2.5 Patient and public involvement
The INTERGROWTH-21
st Steering Committee included voluntary lay member representation during the design and implementation of the project [
44
Ethical issues arising from the INTERGROWTH-21st Fetal Growth Longitudinal Study.
]. We plan to involve pregnant women in the dissemination of results through publication in peer-reviewed journals, presentation at national conferences and involvement of maternity groups associated with the Nuffield Department of Women’s & Reproductive Health, University of Oxford, and the WHO constituted Guideline Development Group – Anaemia: use and interpretation of Hb concentrations for assessing anaemia status in individuals and populations.
2.6 Ethical approval
The INTERGROWTH-21st Project was approved by the Oxfordshire Research Ethics Committee “C” (reference: 08/H0606/139), the research ethics committees of the individual institutions and the regional health authorities where the project was implemented. All women provided informed written consent to participate in the study.
2.7 Role of the funding source
The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
4. Discussion
The gestational age-specific centiles for maternal Hb presented here, are based on a population-based, prospective study throughout pregnancy of 3502 healthy, well-nourished women from eight countries, whose healthy babies were followed up to 2 years of age. The methods for selecting the sample of women adhered strictly to the WHO prescriptive approach used for the construction of the WHO Child Growth Standards [
24
Rationale for developing a new international growth reference.
,
36
- de Onis M.
- Garza C.
- Victora C.G.
- Onyango A.W.
- Frongillo E.A.
- Martines J.
The WHO multicentre growth reference study: planning, study design, and methodology.
], which supports the universal applicability of our findings.
Despite the many factors affecting Hb concentrations, we found remarkable similarities among populations compared with a large within-population variability, in common with other biomarkers of nutritional status [
28
- Villar J.
- Papageorghiou A.T.
- Pang R.
- Ohuma E.O.
- Cheikh Ismail L.
- Barros F.C.
- et al.
The likeness of fetal growth and newborn size across non-isolated populations in the INTERGROWTH-21st Project: the fetal growth longitudinal study and newborn cross-sectional study.
,
42
Group WMGRS
Assessment of differences in linear growth among populations in the WHO multicentre growth reference study.
,
47
- Habicht J.P.
- Martorell R.
- Yarbrough C.
- Malina R.M.
- Klein R.E.
Height and weight standards for preschool children. How relevant are ethnic differences in growth potential?.
]. We also observed a moderate nadir of maternal Hb between 31 and 32 weeks’ gestation as previously reported. The nadir by 31 weeks’ gestation resulted from a drop of 6.8 g/L at the 50th centile compared to values at 14 weeks’ gestation, which is similar to the drop from
13
Recommendations to prevent and control iron deficiency in the United States. Centers for disease control and prevention. MMWR Recommendations and reports: Morbidity and mortality weekly report Recommendations and reports. 1998;47(Rr–3):1–29.
,
14
WHO
WHO recommendations on antenatal care for a positive pregnancy experience.
].
To our knowledge, these are the first normative ranges of Hb values in pregnancy compatible with good, functional, maternal and perinatal outcomes, as well as neonatal and early childhood morbidity, growth and development up to 2 years of age. The 3rd – 97th centile range for maternal Hb is large across gestational ages (around 94 to 141 g/L) clearly demonstrating that healthy pregnant women have adaptive mechanisms to achieve adequate health outcomes within a wide range of Hb values. The resource should, therefore, act as a simple narrative to communicate to mothers the meaning of their routine blood test results.
This work also provides a system, at the individual level, for defining normal Hb distributions based on gestational age-specific cut-offs (
rd centile = low Hb concentration; 3rd – 4.99
th centile = high risk of low Hb concentration; 5
th – 9.99
th centile = moderate risk of low Hb concentration; ≥10
th centile = normal Hb concentration), an approach that is well accepted in biology and medicine. In addition, previous studies have suggested that high haemoglobin concentrations may be associated with increased pregnancy risks, including antepartum stillbirth and pre-eclampsia [
48
- Stephansson O.
- Dickman P.W.
- Johansson A.
- Cnattingius S.
Maternal hemoglobin concentration during pregnancy and risk of stillbirth.
,
49
- Knottnerus J.A.
- Delgado L.R.
- Knipschild P.G.
- Essed G.G.M.
- Smits F.
Haematologic parameters and pregnancy outcome a prospective cohort study in the third trimester.
]. However, these findings are inconsistent, and in part this may be due to using a fixed cut-offs for defining haemoconcentration despite different gestational ages at the time of blood sampling. We believe that studies in this field can be facilitated by our work by allowing uniformity in gestational-age specific definitions of both low and high haemoglobin concentrations.
In short, the results presented here provide an international definition of low Hb concentrations in pregnancy, as well as a strong basis for constructing an international, pregnancy-specific, early warning score system to facilitate earlier recognition of deteriorating health in pregnant women. Our work in conjunction with other studies, that associate Hb concentrations with hypoxia-related outcomes [
50
- Young M.F.
- Oaks B.M.
- Tandon S.
- Martorell R.
- Dewey K.G.
- Wendt A.S.
Maternal hemoglobin concentrations across pregnancy and maternal and child health: a systematic review and meta-analysis.
,
51
- Woodman A.
- Mansour Y.
- Bourque S.
Consequences of maternal iron-deficiency: fetal anemia, and hypoxia in select tissues of the conceptus.
,
52
Significance of an abnormally low or high hemoglobin concentration during pregnancy: special consideration of iron nutrition.
], may provide data to create Hb concentration cut-offs for diagnosing anaemia at population level, although it will be necessary to establish which centiles reflect the different levels (mild, moderate or severe) of this important public health problem. The severity of anaemia determined by Hb concentration also needs to be determined on the basis of adverse outcomes, such as post-partum haemorrhage, the need for transfusion, or maternal or perinatal mortality.
Some thresholds recommended by WHO during pregnancy were proposed in 1958 and revised in 1968 after technical meetings with clinical and public health experts working with the evidence available at the time [
11
WHO Scientific Group on Nutritional Anaemias & World Health Organization
Nutritional anaemias: report of a WHO scientific group [meeting held in Geneva from 13 to 17 March 1967].
]. Those reports relied mostly on data aggregated from four European studies with very small sample sizes (UK, n = 45; Sweden, n = 50; Finland, n = 32; Finland, n = 267) [
11
WHO Scientific Group on Nutritional Anaemias & World Health Organization
Nutritional anaemias: report of a WHO scientific group [meeting held in Geneva from 13 to 17 March 1967].
,
16
- Puolakka J.
- Janne O.
- Pakarinen A.
- Jarvinen P.A.
- Vihko R.
Serum ferritin as a measure of iron stores during and after normal pregnancy with and without iron supplements.
–
20
CDC criteria for anemia in children and childbearing-aged women. MMWR Morbidity and mortality weekly report. 1989;38(22):400–4.
]. Given the limited representativeness of those data and the scientific advances since made in understanding Hb biology [
53
Anemia: progress in molecular mechanisms and therapies.
], the ongoing WHO project on anaemia cut-offs will provide evidence-based guidance on Hb cut-offs for individuals and populations. The results from our work could help to build the body of evidence needed to help WHO to develop guidance for individual and public health programmes and policies.
To our knowledge, this is the first population-based study to collect prospective data from across the world using the prescriptive approach recommended by WHO for the construction of international standards for human growth and development [
24
Rationale for developing a new international growth reference.
]. A prescriptive approach shows how growth should occur, independent of time and place [
54
- Bertino E.
- Milani S.
- Fabris C.
- De Curtis M.
Neonatal anthropometric charts: what they are, what they are not.
]. For human growth, this is usually based on selected populations considered to be of optimal health, for example, with adequate nutritional status and at low risk of abnormal growth. In contrast, the descriptive approach is usually based on an unselected population with minimal exclusion criteria such as known risk factors for optimal health [
55
- Villar J.
- Altman D.G.
- Purwar M.
- Chamberlain P.
- Noble A.
- Knight H.
- Ruyan P.
- Cheikh Ismail L.
- Barros F.
- Lambert A.
- Papageorghiou A.
- Carvalho M.
- Jaffer Y.
- Bertino E.
- Gravett M.
- Bhutta Z.
- Kennedy S.
The objectives, design and implementation of the multicentre, population-based, INTERGROWTH-21st Project.
,
56
Design and other methodological considerations for the construction of human fetal and neonatal size and growth charts.
]. We adopted a robust statistical methodology [
39
Statistical methodology for constructing gestational age-related charts using cross-sectional and longitudinal data: the INTERGROWTH-21st Project as a case study.
,
56
Design and other methodological considerations for the construction of human fetal and neonatal size and growth charts.
], as used in all the integrated studies of the INTERGROWTH-21st Project [
28
- Villar J.
- Papageorghiou A.T.
- Pang R.
- Ohuma E.O.
- Cheikh Ismail L.
- Barros F.C.
- et al.
The likeness of fetal growth and newborn size across non-isolated populations in the INTERGROWTH-21st Project: the fetal growth longitudinal study and newborn cross-sectional study.
,
39
Statistical methodology for constructing gestational age-related charts using cross-sectional and longitudinal data: the INTERGROWTH-21st Project as a case study.
], to pool our data and construct smoothed centiles that provide international gestational age-specific centiles for maternal Hb in healthy pregnancy.
By adopting a prescriptive approach for population selection and a pragmatic, yet highly standardised, approach to the design of the study, that mimics routine clinical practice in each of the eight diverse sites, we are confident that the international centiles are both statistically robust and representative of adult women of optimal health, nutrition, education, and socioeconomic status with uncomplicated pregnancies. Therefore, these Hb centiles represent normative values that public health measures should be targeted at achieving.
The proportion of total variance attributed to population differences among sites was only <13%, supporting the position that population-specific ranges for maternal Hb in pregnancy are not required. Furthermore, despite the great reduction in sample size when modelling Hb data for a single site separately, it was evident that there is less inter-site variation, and more so at the 3rd centile. Our findings are further strengthened by the accuracy of gestational age estimation in the study cohort, all of whom had a confirmatory dating scan before 14 weeks’ gestation.
The study has some limitations. Firstly, we do not provide values for non-pregnant women. Secondly, we lacked pre-pregnancy and maternal Hb data <14 weeks’ gestation; however, a pre-pregnancy measure is rarely available in routine clinical practice so comparison with maternal Hb in early pregnancy has greater clinical applicability. Thirdly, because we took a pragmatic approach to the study design in relation to laboratory tests, we relied on collecting the results of available routine blood tests. The commercially available instruments for assessing Hb were not standardised across sites, however, all laboratories underwent standard laboratory quality assurance. Information on the use of preventive or therapeutic iron and folic acid supplements was collected from medical records. However, based on descriptive analyses, the risk of large systematic method differences was small. Fourthly, we do not provide values for women living in in high altitudes >1600 m. Lastly, the sample size, though large for a prospective study with repeated measures, the purposive selection of healthy women resulted in a relatively small sample to explore associations with maternal and neonatal outcomes such as preeclampsia.
The new Hb centiles allow comparisons across countries and regions using the same definitions and thresholds for potential interventions at population level, so as to harmonise efforts by WHO and other public health organisations to prevent and treat nutritional anaemias. Given the importance of evidence-informed interventions to improve maternal and child nutrition [
57
- Bhutta Z.A.
- Das J.K.
- Rizvi A.
- Gaffey M.F.
- Walker N.
- Horton S.
- et al.
Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost?.
], we believe that national and international guidelines on antenatal care should take account of our findings. The fact that the centiles are gestational age-specific should also encourage policymakers to ensure that the gestational age of every pregnancy is estimated as accurately as possible, in line with the WHO 2016 guidelines [
14
WHO
WHO recommendations on antenatal care for a positive pregnancy experience.
].
Clearly, compared to the current recommendation [
13
Recommendations to prevent and control iron deficiency in the United States. Centers for disease control and prevention. MMWR Recommendations and reports: Morbidity and mortality weekly report Recommendations and reports. 1998;47(Rr–3):1–29.
,
14
WHO
WHO recommendations on antenatal care for a positive pregnancy experience.
], the derived haemoglobin distributions may have major policy implications because, once implemented, fewer pregnant women may be diagnosed with anaemia and the prevalence of low Hb levels will be substantially lower. This arises for two main reasons. Firstly, the current definition is derived from a statistical approach based on four very small studies, whereas the new derived haemoglobin distributions are compatible with the levels of functional health outcomes observed in the healthy populations we studied; secondly, we are presenting Hb trajectories according to gestational age rather than a single fixed cut-off across the whole of pregnancy (Fig. 4), which is an implausible biological concept. However, lowering the threshold for defining anaemia towards the end of pregnancy at individual level might have implications for management; for instance, recognising lower thresholds may allow more targeted treatment for anemia, and may alter management in those women who then have a post-partum haemorrhage.
Finally, considering the indisputable need for pregnancy-specific early warning scores that incorporate maternal Hb changes [
3
- Pasricha S.R.
- Colman K.
- Centeno-Tablante E.
- Garcia-Casal M.N.
- Pena-Rosas J.P.
Revisiting WHO haemoglobin thresholds to define anaemia in clinical medicine and public health.
,
22
- Garcia-Casal M.N.
- Pasricha S.R.
- Sharma A.J.
- Pena-Rosas J.P.
Use and interpretation of hemoglobin concentrations for assessing anemia status in individuals and populations: results from a WHO technical meeting.
] our findings could be used to facilitate earlier recognition and treatment of the unwell pregnant woman and thereby reduce both maternal morbidity and mortality rates worldwide.
Future research that focuses on obtaining accurate data on plasma volume expansion (using non-invasive methods) during healthy pregnancies would be ideal as this parameter has an impact on many biomarkers in pregnancy. Based on these derived gestation-specific centiles, a study that evaluates the statistically derived cut-offs including upper limit cut-offs and the perinatal risk-associated cut-off levels using large datasets with sufficient severe morbidity and mortality events would help to establish and validate the derived thresholds and would add support to more evidence-based protocols for the care of pregnant women.
To our knowledge, this is the first attempt to produce maternal Hb thresholds based on populations selected using the WHO prescriptive approach for the construction of international standards. We present international, gestational age-specific centiles for Hb in pregnancy, which are compatible with good, functional, maternal and perinatal outcomes, as well as neonatal and early childhood morbidity, growth and development up to 2 years of age.
Funding
This study was supported by the Bill & Melinda Gates Foundation. The funders were not involved in the analysis or writing of the study. This work was commissioned and financially supported by the Evidence and Programme Guidance Unit, Department of Nutrition for Health and Development, WHO, Geneva, Switzerland. EOO received an honorarium from WHO for this work. The WHO BMGF award that funded anaemia was 64662 (2016-2019). USAID has funded anaemia through various awards this year (69730, 69278, 70209).
Author contributions
JV and SHK were responsible for conceiving the INTERGROWTH-21st Project. JPPR and MNGC conceived the protocol in collaboration with EOO and JV. EOO performed the statistical analyses on the maternal Hb data in collaboration with JV. EOO wrote the paper in collaboration with JV, MY, RM, MdO and SHK with input from all co-authors. All co-authors read the report and made suggestions about its content.
Acknowledgments
We would like to thank the Health Authorities in Pelotas, Brazil; Beijing, China; Nagpur, India; Turin, Italy; Nairobi, Kenya; Muscat, Oman; Oxford, UK and Seattle, USA, who facilitated the project by allowing participation of these study sites as collaborating centers. We are extremely grateful to Philips Medical Systems who provided the ultrasound equipment and technical assistance throughout the project. We also thank MedSciNet UK Ltd for setting up the INTERGROWTH-21st web-site and for the development, maintenance and support of the on-line data management system.
We thank the parents and infants who participated in the studies and the more than 200 members of the research teams who made the implementation of this project possible. The participating hospitals included: Brazil, Pelotas (Hospital Miguel Piltcher, Hospital São Francisco de Paula, Santa Casa de Misericórdia de Pelotas, and Hospital Escola da Universidade Federal de Pelotas); China, Beijing (Beijing Obstetrics & gynecology Hospital, Shunyi Maternal & Child Health Centre, and Shunyi General Hospital); India, Nagpur (Ketkar Hospital, Avanti Institute of Cardiology Private Limited, Avantika Hospital, Gurukrupa Maternity Hospital, Mulik Hospital & Research Centre, Nandlok Hospital, Om Women’s Hospital, Renuka Hospital & Maternity Home, Saboo Hospital, Brajmonhan Taori Memorial Hospital, and Somani Nursing Home); Kenya, Nairobi (Aga Khan University Hospital, MP Shah Hospital and Avenue Hospital); Italy, Turin (Ospedale Infantile Regina Margherita Sant’ Anna and Azienda Ospedaliera Ordine Mauriziano); Oman, Muscat (Khoula Hospital, Royal Hospital, Wattayah Obstetrics & Gynaecology Poly Clinic, Wattayah Health Centre, Ruwi Health Centre, Al-Ghoubra Health Centre and Al-Khuwair Health Centre); UK, Oxford (John Radcliffe Hospital) and USA, Seattle (University of Washington Hospital, Swedish Hospital, and Providence Everett Hospital).
Full acknowledgement of all those who contributed to the development of the INTERGROWTH-21st Project protocol appears at
www.intergrowth21.org.ukData sharing statement
All documentation, protocols, data collection forms, and clinical tools are freely available on the INTERGROWTH-21st website
www.intergrowth21.org.uk. EOO guarantees that the manuscript is an honest, accurate, and transparent account of the study being reported and that no aspects have been omitted.

{kind=link}