Preterm birth (PTB) and small for gestational age (SGA) are increasingly prevalent, with major consequences for health and development into later life. There is emerging evidence that some risk processes begin before pregnancy. We report on associations between maternal and paternal common mental disorders (CMD) before and during pregnancy and offspring PTB and SGA.
Methods
398 women with 609 infants and 267 men with 421 infants were assessed repeatedly for CMD symptoms before pregnancy between age 14 and 29 and during pregnancy. Associations between preconception and antenatal CMD symptoms and offspring gestational age/PTB and size for gestational age/SGA were estimated using linear and Poisson regression.
Findings
In men, persistent preconception CMD across adolescence and young adulthood predicted offspring PTB after adjustment for ethnicity, education, BMI and adolescent substance use (adjusted RR 7·0, 95% CI 1·8,26·8), corresponding to a population attributable fraction of 31% of preterm births. In women, antenatal CMD symptoms predicted offspring PTB (adjusted RR 4·4, 95% CI 1·4,14·1). There was little evidence of associations with SGA.
Interpretation
This first report of an association between paternal preconception mental health and offspring gestational age, while requiring replication in larger samples, complements earlier work on stress in animals, and further strengthens the case for expanding preconception mental health care to both men and women.
Funding
National Health and Medical Research Council (Australia), Victorian Health Promotion Foundation, Australian Rotary Health, Colonial Foundation, Perpetual Trustees, Financial Markets Foundation for Children (Australia), Royal Children’s Hospital Foundation, Murdoch Children’s Research Institute, Australian Research Council.
1. Introduction
Preterm birth (PTB) and small for gestational age (SGA) are leading causes of neonatal morbidity and mortality [
The epidemiology, etiology, and costs of preterm birth.
]. SGA is also associated with increased risk for neonatal morbidity and mortality, as well as short- and long-term adverse health outcomes and functional impairment, with these effects attributable primarily to fetal growth restriction [
] but these only explain a small proportion of variance in PTB and SGA and preventive intervention efforts based on these risk factors are estimated to reduce PTB rates by only 5% [
]. In experimental animal research, parental preconception stress has been linked to offspring development via enduring effects on parental reproductive biology [
Extending the developmental origins of disease model: impact of preconception stress exposure on offspring neurodevelopment.
]. These findings point to an influence of preconception stress on offspring development even in the absence of antenatal exposure. There is some suggestion in humans that links between antenatal maternal mental disorder and offspring PTB may originate in the years immediately prior to pregnancy [
Prediction of perinatal depression from adolescence and before conception (VIHCS): 20-year prospective cohort study.
]. Investigating contributions of mental health problems, from adolescence to parenthood, to offspring birth outcomes may help elucidate mechanisms and identify possible intervention points. For example, the timing and persistence of any effects may implicate either sensitive periods or chronicity. Effects of exposure before, but not during, pregnancy may indicate direct preconception effects on parental reproductive biology, or mediation through other antenatal pathways [
Mechanisms of non-genetic inheritance and psychiatric disorders.
]. Effects of parental mental disorder both before and during pregnancy may suggest effects of exposure at each phase via differing mechanisms, or confounding by underlying genetic or environmental influences of the association between mental disorder and offspring PTB or SGA [
Spontaneous preterm birth and single nucleotide gene polymorphisms: a recent update.
]. Comparison of maternal and paternal associations is a further approach to investigating confounding effects of shared genes and environment, under the assumption that maternal and paternal exposures are similarly confounded [
Negative control exposures in epidemiologic studies.
].
Here, we used a two-generation cohort study with prospective data on maternal and paternal mental disorder over 15 years from adolescence to young adulthood, and again during pregnancy. We aimed to examine the association between maternal and paternal symptoms of common mental disorders (CMD) from adolescence to parenthood and offspring birth outcomes of PTB or SGA and whether these associations differ by timing of parental CMD symptoms and parent exposed.
5. Results
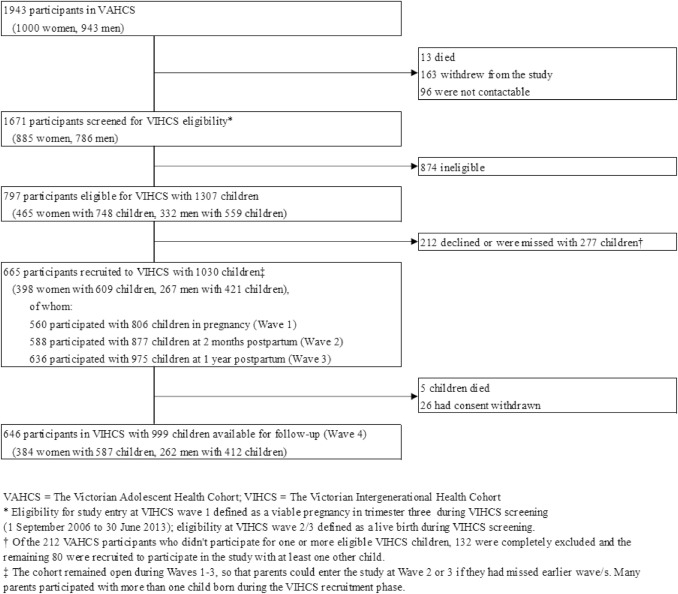
Our sample included 398 women with 609 children and 267 men with 421 children. The flow of participants through VIHCS is presented in Fig. 1. Demographics of those screened for, identified as eligible for and participating in VIHCS broadly matched those of the original adolescent cohort (VAHCS) [
The Victorian Intergenerational Health Cohort Study (VIHCS): study design of a preconception cohort from parent adolescence to offspring childhood.
]. Basic demographics of the sample and proportion of missing data in each variable are presented in Table 1. Approximately one half of women and one quarter of men had CMD symptoms in at least one of the adolescent study waves, with similar proportions seen during the young adult waves; 27% of women and 11% of men had CMD symptoms persisting across both adolescence and young adulthood, while 11% of both women and men had symptoms during pregnancy at 32 weeks gestation. Of those with complete birth outcome data, approximately 6% of both women and men had babies who were either preterm or SGA.
Fig. 1Sampling of the Victorian Intergenerational Health Cohort Study (VIHCS), from 2006 to 2014.
Table 1Characteristics of the cohort (N = 1030), by sex of parent.
The unadjusted and adjusted associations between the two exposures of preconception and antenatal CMD symptoms and birth outcomes for women, using imputed data are shown in Table 2. There was evidence of an association between antenatal CMD symptoms and PTB, with maternal symptoms increasing PTB risk (relative risk (RR) 3·5; 95% confidence interval (CI) 1·3,9·1); this association remained after adjustment for the woman’s parents’ high school completion, ethnicity, preconception CMD symptoms, overweight or underweight in adolescence and smoking and binge drinking in adolescence (adjusted RR 4·4; 95% CI 1·4,14·1). Assuming that this estimate reflects the magnitude of the true causal effect, this increased risk translates to a reduction in PTB by as much as 13% (the population attributable fraction), had no women experienced antenatal CMD symptoms. When gestational age at birth was considered as a continuous variable, this effect was in the same direction. Little evidence was found for an association between preconception or antenatal CMD symptoms and SGA, as either a binary or continuous outcome.
Table 2Associations between preconception and antepartum symptoms of CMD with gestational age and size for gestational age in infants from women (N = 609).
Imputed models using Poisson or linear regression within a generalised estimating equation framework with robust standard errors.
In men (Table 3), there was evidence of an association between preconception CMD symptoms and PTB, with persistent CMD symptoms across adolescence and young adulthood showing the greatest magnitude (RR 8·8; 95% CI 2·4,32·2). This remained after adjustment (adjusted RR 7·0; 95% CI 1·8,26·8) and when gestational age at birth was considered as a continuous variable (unadjusted beta −0·8; 95% CI −1·5,−0·1 and adjusted beta −0·8; 95% CI −1·5,−0·01), translating to an earlier gestational age of around five days in men exposed to persistent preconception CMD symptoms compared with those without preconception symptoms. The corresponding population attributable fraction is 31%. There was little evidence of an association between paternal preconception or antenatal CMD symptoms and SGA and between paternal antenatal CMD symptoms and PTB, when considered as either a continuous z-score or binary outcome.
Table 3Associations between preconception and antepartum symptoms of CMD with gestational age and size for gestational age in infants from men (N = 421).
Imputed models using Poisson or linear regression within a generalised estimating equation framework with robust standard errors.
Available case analyses yielded a similar pattern of results for both women and men (see Supplementary Table 1 and Supplementary Table 2).
6. Discussion
Infants of men with persistent preconception CMD symptoms were more than six times more likely to be born preterm than infants of men without preconception CMD symptoms. Similarly, mean gestational age at birth among infants exposed to persistent paternal preconception CMD symptoms was almost one week earlier than among unexposed infants. If our estimates reflect the magnitude of the true causal effects, up to 31% of PTBs could be attributable to processes relating to persistent paternal preconception CMD symptoms. We also found an increased risk of PTB among infants exposed to maternal antenatal CMD symptoms, corresponding to a population attributable fraction of 13% of PTBs; these findings are consistent with earlier reports [
A meta-analysis of depression during pregnancy and the risk of preterm birth, low birth weight, and intrauterine growth restriction.
]. However, evidence of an association between paternal preconception CMD and offspring PTB has not previously been reported. These paternal associations persisted after adjustment for potential paternal socioeconomic, substance use, and BMI confounders. Thus this study provides a first indication that men’s CMD symptoms in the decades prior to conception are associated with offspring PTB: an early life marker of disease and developmental risk.
The prevalence of preconception CMD symptoms in our study was similar to that previously reported in other prospective cohorts [
Several mechanisms may explain the association between maternal antenatal CMD symptoms and offspring PTB. We accounted for a number of background factors and maternal characteristics that might increase risk of both maternal CMD symptoms and PTB, including family of origin demographics such as education and ethnicity, substance use, prior preconception CMD symptoms, and BMI. There remains potential for residual confounding, including lifetime experience of interpersonal violence or unplanned pregnancy [
Does a maternal history of abuse before pregnancy affect pregnancy outcomes? A systematic review with meta-analysis.
]. There are also a number of potential mediators of these associations which warrant further investigation in larger samples. These include antidepressant use during pregnancy (although increased risk for PTB has also been found in those with untreated antenatal depression [
A meta-analysis of depression during pregnancy and the risk of preterm birth, low birth weight, and intrauterine growth restriction.
]. Antenatal CMD symptoms may also lead to adverse birth outcomes through impacts on maternal endocrine and immune functioning, all implicated in PTB [
Maternal hypothalamus-pituitary-adrenal (HPA) system activity and stress during pregnancy: effects on gestational age and infant’s anthropometric measures at birth.
].
We did not find evidence of preconception maternal effects. Prior findings are mixed; those studies reporting preconception associations have mostly assessed preconception stress exposure closer to the time of conception [
Preconception Mental Health Predicts Pregnancy Complications and Adverse Birth Outcomes: a National Population-Based Study.
] so may better reflect antenatal effects. Evidence in this study for maternal antenatal associations but not maternal preconception or paternal antenatal, provide some further support for a potential causal effect of stress-related intrauterine processes.
There are similarly a range of processes by which paternal preconception CMD symptoms may be associated with offspring PTB. One possibility is residual confounding by early life characteristics, such as childhood maltreatment [
Does childhood trauma influence offspring’s birth characteristics?.
]. A further potential explanation is that the risk from paternal preconception CMD symptoms is mediated through maternal antenatal factors. Assortative mating is a tendency to choose partners with similar characteristics and has been observed in couples affected by CMD [
Patterns of nonrandom mating within and across 11 major psychiatric disorders.
]. Partners of men with CMD are also at increased risk of exposure to other risk factors for adverse birth outcomes, including socioeconomic adversity, tobacco smoke exposure, and intimate partner violence [
Perpetration of intimate partner violence by people with mental illness.
].
Associations between persistent preconception CMD symptoms in men and infant PTB may also be mediated by paternal processes occurring in the months immediately before conception. In the testes, the production of new sperm cells from germ cells begins at puberty and continues throughout life. Production of each sperm cell takes around three months and is affected by environmental exposures, including substance use, poor nutrition, and exposure to environmental toxins, which are associated with both paternal CMD and offspring development [
Before the beginning: nutrition and lifestyle in the preconception period and its importance for future health.
].
Given the dose-response relationship between preconception CMD symptoms and offspring PTB, a further possibility is that chronic or recurrent CMD in the preconception years may have direct, cumulative and enduring effects on the male reproductive tract. There is some precedent for this proposal in the animal literature [
Mechanisms of non-genetic inheritance and psychiatric disorders.
], although it has been little examined in humans. The pre-puberty period, with the formation of blood-testis and blood-epididymis barriers and commencement of spermatogenesis, has also been implicated as a sensitive window during which exposures may have a greater influence on reproductive development [
Environmental susceptibility of the sperm epigenome during windows of male germ cell development.
]. In our study, strong associations were observed between offspring PTB and paternal preconception but not antenatal CMD symptoms. These findings raise the possibility of sensitivity of the male germline to stress, not limited to the immediate preconception window but beginning in late childhood and extending into adolescence.
We did not find evidence of an association between preconception or antenatal CMD symptoms and offspring SGA in either women or men. These findings are consistent with results of prior meta-analyses [
Correlates of anxiety symptoms during pregnancy and association with perinatal outcomes: a meta-analysis.
]. One potential contributor is the biological heterogeneity of SGA, which comprises both constitutional differences attributable to genetic factors and processes relating to fetal growth restriction. Capturing these subtypes of SGA would require repeated assessments of fetal growth, beyond this study’s scope. It remains possible that parental CMD may influence fetal growth restriction.
Strengths of this study include the repeated assessment of CMD symptoms across 15 years from adolescence to young adulthood and during subsequent pregnancies. Some limitations should also be noted. While we attempted to control for baseline confounders associated with both CMD and adverse birth outcomes, it is also possible that there is some residual confounding from unmeasured socio-environmental risks such as early life trauma, interpersonal violence, and socioeconomic adversity. Nonetheless, our finding of different maternal and paternal associations also suggest that results are not entirely attributable to familial confounding, under the assumption that maternal and paternal CMD symptoms are similarly confounded [
Negative control exposures in epidemiologic studies.
]. Infant birth outcomes were assessed by maternal report, which may be subject to reporting bias, although prior studies have found good agreement between maternal report and medical records of birthweight and gestational age at birth, particularly when continuous data are collected and when reported in the postpartum or early childhood [
Medical record validation of maternally reported birth characteristics and pregnancy-related events: a report from the Children’s Cancer Group.
]. In our study, most birth outcome data were collected at two months postpartum, with a smaller proportion collected at one year postpartum (3%) or the following VAHCS wave (11%, mean child age 3.8 years). This study was limited to infants born when parents were aged between 29 and 35 years. This design allowed us to maximise recruitment across the period of peak fertility in Australia but results may not be generalisable to older or younger parents with different risk profiles.
As with all cohort studies, the possibility of differential recruitment, attrition and non-response, and changing population demographics over time may have led to underrepresentation of some population groups. VAHCS maintains a high retention rate, and 85% of those with live births during screening participated in VIHCS. The retained and participating samples were broadly representative of the baseline VAHCS and eligible VIHCS samples respectively on measured baseline characteristics, but may differ on unmeasured confounders. Similarly, we were unable to examine associations within specific population groups known to have higher rates of preterm births, such as Aboriginal and Torres Strait Islander peoples [
Australian Institute of Health and Welfare Australia mothers and babies 2015 – perinatal dynamic data displays.
], and this remains an area for future research. The sample in this study was relatively small, reducing precision of our estimates; findings should be interpreted as preliminary, and need replication in larger or pooled samples with similarly strong longitudinal designs. Missing data were low at each preconception and postpartum wave, but higher antenatally due to challenges of detecting all pregnancies before birth. We addressed potential biases arising from missing data using multiple imputation and the conclusions were unaltered.
Life course epidemiology and public health policy have long been grounded in assumptions around the causal primacy of maternal exposures and those occurring during pregnancy and early life [
It’s the mother!: how assumptions about the causal primacy of maternal effects influence research on the developmental origins of health and disease.
]. While maternal antenatal risk factors for adverse birth outcomes remain an important focus for intervention, findings of the current study join a growing body of evidence highlighting the relevance of both paternal exposures and those prior to conception for offspring outcomes [
Before the beginning: nutrition and lifestyle in the preconception period and its importance for future health.
]. Given the high prevalence of CMD and the known adverse outcomes of PTB, the potential public health impact of their relationship is substantial. Our findings require replication in larger and diverse samples, with further examination of the mechanisms by which paternal persistent preconception CMD symptoms and maternal antenatal CMD symptoms might influence offspring PTB. Whether mediated by biological or psychosocial processes, our findings support calls for an expansion of preconception care to include strategies to address CMD, for both men and women [
The clinical content of preconception care: preconception care for men.
]. The findings also underscore the importance of optimising mental health in adolescence and young adulthood, prior to pregnancy, emphasising the need for investment in coordinated care between child and adolescent, adult and specialist perinatal mental health services [
Public Health England Making the case for preconception care.
]. Intervention in adolescence to prevent onset and persistence of CMD into adulthood and pregnancy is likely to yield benefits not only for parents’ own continuing mental health, but also for the development of their children, either by preventing the potential direct impact of preconception CMD on offspring birth outcomes or interrupting potentially more complex developmental risk trajectories.


{kind=link}