Abbreviations
-
- ANOVA
-
- analysis of variance
-
- BMI
-
- body mass index
-
- BSFS
-
- Bristol Stool Form Scale
-
- ENT
-
- ear, nose, throat
-
- FD
-
- functional Dyspepsia
-
- FGIDs
-
- functional gastrointestinal disorders
-
- FH
-
- functional heartburn
-
- GAD7
-
- generalized anxiety disorder 7
-
- GI
-
- gastrointestinal
-
- HPAa
-
- hypothalamic‐pituitary‐adrenal axis
-
- IBS
-
- irritable bowel syndrome
-
- IQR
-
- interquartile range
-
- MERS
-
- Middle East respiratory syndrome
-
- MS
-
- multiple sclerosis
-
- PSS10
-
- Perceived Stress Scale 10
-
- SAMs
-
- sympathetic‐adrenal‐medullary system
-
- SARS
-
- severe acute respiratory syndrome
-
- SD
-
- standard deviation
Key Points
- Psychological stress and anxiety could affect gastrointestinal symptoms course in patients with functional gastrointestinal disorders.
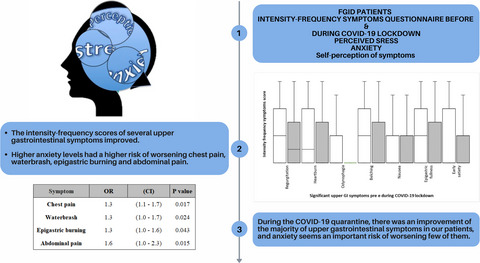
- During COVID‐19 lockdown the intensity‐frequency scores of several upper gastrointestinal symptoms improved.
- Higher anxiety levels had a higher risk of worsening chest pain, waterbrash, epigastric burning and abdominal pain.
1 INTRODUCTION
The outbreak of COVID‐19, which started in the Chinese province of Hubei over the last months of 2019, has quickly spread throughout the world, forcing affected nations to adopt restrictive measures and forced quarantine, which has, therefore, resulted in a great limitation on individual freedom. In Italy, the restrictive measures due to the widespread outbreak of COVID‐19 culminated in the complete national lockdown established on March 9th, 2020.
Psychological stress conditions and high anxiety levels, linked to the forced quarantine, have been deeply described in several studies related to the effects of previous viral outbreaks (Severe Acute Respiratory Syndrome [SARS] and Middle East Respiratory Syndrome [MERS]) on mental health.1, 2 Previous works underlined how stressful life events could trigger affective responses, such as worry, fear, and anxiety, activating the Hypothalamic‐Pituitary‐Adrenal (HPAa) axis, Sympathetic‐Adrenal‐Medullary (SAMs) system, and regulatory neuroendocrine systems, finally causing diseases onset and deterioration of the clinical course.3, 4
In this context, Functional Gastrointestinal Disorders (FGIDs) fit perfectly. FGIDs are syndromes based on upper and/or lower gastrointestinal (GI) symptoms that cluster together and are diagnosed by Rome IV criteria, only after excluding organic or structural underlying disorders.5
The presence and reciprocal interactions among social, psychological, and biological factors are necessary conditions for the FGID development and maintenance.5 Prospective studies have demonstrated that among environmental stressors that have been linked to FGID, the experience of stressful life events is associated with symptom exacerbation and frequent healthcare seeking among adults with irritable bowel syndrome (IBS).6
Mood disorders such as depression and anxiety occur in most of FGID patients, conditioning GI symptoms onset and maintenance through their associated heightened autonomic arousal (in response to stress) or at the level of the brain, which can interfere with GI sensitivity and motor function.7–11
Previous studies showed how stress conditions, anxiety and depression could increase pain levels in IBS patients, and gastric discomfort in patients with functional dyspepsia (FD), as the result of the alteration of visceral pain stimuli brain processing and of colonic and gastric motility patterns.10, 12–15 The neurophysiological basis of the possible link between FGID and psychological processes and psychiatric comorbidity has been studying extensively, specifically, the critical role of bidirectional signaling mechanisms between the GI tract and the central nervous system.10
To the best of our knowledge, there are no studies investigating the association between psychological distress secondary to COVID‐19 outbreak and FGID symptoms.
Thus, our aim was to assess in a cohort of patients with FGID regularly followed up in a devoted outpatient clinic of the South of Italy the association between their symptom changes and stress and anxiety reported during the Italian national lockdown.
2 MATERIALS AND METHODS
2.1 Participants
For this study, patients from the outpatient clinic of the University of Salerno, devoted to FGID, were recruited. Sixty‐nine patients with Functional Heartburn (FH), FD and/or IBS and its subgroups according to Rome IV criteria,5, 16–18 examined over the last 6 months before the COVID‐19 outbreak, were selected from a prospectively maintained database. Age, gender, weight, height, body mass index (BMI) as well as a number of upper and lower GI symptoms that are routinely collected at each visit using a standardized questionnaire were pooled in a database (T0). On 45th days from the beginning of Italian lockdown, these patients were contacted by a phone call and re‐assessed by gastroenterologists with expertise in FGID for their upper and lower GI symptoms using the same standardized questionnaire (T1). Furthermore, patients who successfully answered to the standardized questionnaire were invited to fill in an online self‐administered internet‐based questionnaires immediately sent by a message with a link via email, WhatsApp, or Facebook.
2.2 Upper and lower GI symptoms questionnaire
A previously published standardized questionnaire dealing with the presence, the frequency from 0 to 3 (0 = absent, 1 = 2 d/wk; 2 = 3–5 d/wk; and 3 = 6 or 7 d/wk) and the intensity from 0 to 3 (0 = absent; 1 = not very bothersome, not interfering with daily activities; 2 = bothersome, but not interfering with daily activities; and 3 = interfering with daily activities), of a number of upper and lower GI symptoms is routinely used in our outpatient clinic.19, 20
Upper GI symptoms such as dysphagia for solids, dysphagia for liquids, regurgitation, heartburn, non‐cardiac chest pain, ENT (ear, nose, throat) symptoms, cough, odynophagia, waterbrash, belching, halitosis, nausea, vomiting, upper abdominal bloating, upper abdominal distension, epigastric fullness, early satiety, epigastric pain and epigastric burning and lower GI symptoms such as abdominal pain, the sensations of incomplete evacuation, effort during evacuation, anal blockage, usage of digital and/or manual maneuvers to facilitate evacuation, lower abdominal bloating, visible lower abdominal distension, flatulence, urgency, incontinence were collected. For each symptom, a frequency‐intensity score from 0 up to a maximum of 6 was obtained. Stool consistency was recorded as numerical values using the Bristol Stool Form Chart Adjectival scale for stool consistency (BSFS).21 Daily measurement of the number of bowel movements was summarized weekly.22
2.3 Online self‐administered questionnaires
Two self‐administered, internet‐based structured questionnaires on Google platform were sent to measure anxiety and stress. The opening page of the survey provided information about the scope and purpose of the study and contained mandatory patient consent. Firstly, they were asked to answer the following question online: “Compared to the interval preceding the COVID‐19 outbreak, how would you score your symptoms?” (1 = extremely worsened; 2 = worsened; 3 = unchanged; 4 = improved; 5 = extremely improved).
Anxiety levels were evaluated by the Generalized Anxiety Disorder (GAD‐7) test, a 7‐item questionnaire that asked patients how often, during the last two weeks, each symptom had been bothering them. The following option answers: “not at all,” “several days,” “more than half the days,” and “nearly every day”, scored as 0, 1, 2, and 3.23 For its accuracy, GAD‐7 is an approved “gold standard” tool, based on an internationally recognized diagnostic system.24 A score of 8 or more on the GAD‐7 is a cutoff for cases of GAD.
Stress levels were evaluated by the Perceived Stress Scale 10 (PSS‐10) test. The PSS evaluates the degree to which an individual perceived life as unpredictable, uncontrollable, and overloading in the previous month. The PSS consists of 10‐items that were rated on a five‐point response scale (0 = never, 1 = almost never, 2 = sometimes, 3 = fairly often, 4 = very often). All item scores must be combined to produce a total score in the range 0–40. A high score indicates a high degree of perceived stress, and no cutoffs were predefined.25–27
2.4 Outcome parameters
The primary outcome was the impact of perceived stress and anxiety on upper and lower GI symptom changes before and during late COVID‐19 outbreak.
Secondary outcome was the response to the question, “Compared to the interval preceding the COVID‐19 outbreak, how would you score your symptoms?” (1 = extremely worsened; 2 = worsened; 3 = unchanged; 4 = improved; 5 = extremely improved) and its association with the level of anxiety measured by GAD‐7 and stress by PSS‐10 in all FGID patients.
2.5 Statistical analysis
Frequencies, median and Interquartile range (IQR) or means and standard deviations for discrete or continuous variables were computed, respectively. When appropriate, a χ2 test to compare categorical data and Analysis of Variance (ANOVA) to compare continuous variables were used. The intensity‐frequency score of each GI symptom before and at 45 days after the Italian lockdown (T0 vs T1) was compared by the Wilcoxon’s test for paired data. Intensity‐frequency scores changes (T1 vs T0) were calculated for each GI symptom and recoded as improved/neutral or worsened.
Logistic regression models were built to assess the relationship between each GI symptom improved/neutral or worsened as dependent variable and age, sex, perceived stress and anxiety level as covariates (Primary Endpoint). The relationship among the level of anxiety, perceived stress, and the patient’s perception of GI symptoms was assessed by a multivariate regression analysis (Secondary Endpoint). Significance was expressed at p < 0.05 level. SPSS for Windows (release 15.0; SPSS Inc.) was used for statistical analysis.
3 RESULTS
Demographic characteristics are shown in Table 1. Sixty‐nine patients agreed to answer the standardized questionnaire to evaluate FGID symptoms and were enrolled. Forty‐four (63.7%) patients filled in the online questionnaires to assess their anxiety and stress levels. There were no significant differences in age, sex, BMI, FGID diagnosis, and any symptom evaluated before lockdown between patients who filled in the online questionnaire and patients who did not (Table 2).
Demographic characteristics, and the prevalence of each FH, FD, and IBS
| Patients | n = 69 |
|---|---|
| Age (years) (M ± SD) | 43 ± 16.7 |
| Sex (n, %) | F 49 (71%) |
| BMI (M ± SD) | 24.8 ± 4.14 |
| FH (n, %) | 18 (26%) |
| FD (n, %) | 30 (43.5%) |
| IBS‐C (n, %) | 8 (11.6%) |
| IBS‐D (n, %) | 13 (18.8%) |
| IBS‐M (n, %) | 4 (5.8%) |
| IBS‐U (n, %) | 3 (4.3%) |
Demographic characteristics, and the prevalence of each FH, FD, and IBS in 25 FGID patients who did not fill in the online questionnaire
| Patients | n = 25 |
|---|---|
| Age (years) (M ± SD) | 45.0 ± 17.9 |
| Sex (n, %) | F 18 (72%) |
| BMI (M ± SD) | 24.7 ± 3.1 |
| FH (n, %) | 9 (36%) |
| FD (n, %) | 10 (40%) |
| IBS‐C (n, %) | 3 (12%) |
| IBS‐D (n, %) | 5 (20%) |
| IBS‐M (n, %) | 0 (0%) |
| IBS‐U (n, %) | 1 (4%) |
None reported symptoms possibly due to SARS‐CoV‐2 infection and none in their family members or cohabitants were diagnosed with COVID‐19. During late COVID‐19 lockdown, the intensity‐frequency scores of regurgitation, heartburn, odynophagia, belching, nausea, epigastric fullness, and early satiety significantly improved compared to the interval before the COVID‐19 outbreak. (Wilcoxon test <0.05 in all cases). The remaining GI symptoms did not reach a statistical significance (Table 3). Figure 1 shows the box plots of upper and lower GI symptom.
GI symptoms before (T0) and during the Covid‐19 lockdown (T1)
| Symptom | Pre ‐ Lockdown | 45 days of Lockdown | p‐Value |
|---|---|---|---|
| Dysphagia for solids | 0.0 (0.0–2.0) | 0.0 (0.0–0.0) | 0.05 |
| Dysphagia for liquids | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.39 |
| Regurgitation | 2.0 (0.0–4.0) | 1.0 (0.0–3.0) | 0.02 |
| Heartburn | 1.0 (0.0–4.0) | 0.0 (0.0–3.0) | 0.02 |
| Non‐cardiac chest pain | 0.0 (0.0–2.0) | 0.0 (0.0–3.0) | 0.72 |
| ENT symptoms | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.05 |
| Cough | 0.0 (0.0–2.0) | 0.0 (0.0–2.0) | 0.40 |
| Odynophagia | 0.0 (0.0–2.0) | 0.0 (0.0–0.0) | 0.00 |
| Waterbrash | 0.0 (0.0–2.0) | 0.0 (0.0–2.0) | 0.39 |
| Belching | 2.0 (0.0–4.0) | 0.0 (0.0–3.0) | 0.01 |
| Halitosis | 1.0 (0.0–2.0) | 0.0 (0.0–2.0) | 0.101 |
| Nausea | 0.0 (0.0–2.0) | 0.0 (0.0–2.0) | 0.00 |
| Vomiting | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.37 |
| Upper abdominal bloating | 2.0 (0.0–4.0) | 2.0 (0.0–4.0) | 0.23 |
| Upper abdominal distension | 0.5 (0.0–4.0) | 0.0 (0.0–3.0) | 0.20 |
| Epigastric fullness | 2.0 (0.0–4.0) | 0.0 (0.0–3.0) | 0.02 |
| Early satiety | 0.0 (0.0–4.0) | 0.0 (0.0–2.0) | 0.03 |
| Epigastric pain | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.56 |
| Epigastric burning | 0.0 (0.0–2.0) | 0.0 (0.0–0.0) | 0.23 |
| Abdominal pain | 1.0 (0.0–2.0) | 0.0 (0.0–2.0) | 0.26 |
| Incomplete evacuation | 0.0 (0.0–4.0) | 0.0 (0.0–3.0) | 0.60 |
| Effort during evacuation | 0.0 (0.0–2.0) | 0.0 (0.0–0.0) | 0.28 |
| Anal blockage | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.40 |
| Maneuvers to evacuate | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.20 |
| Lower abdominal bloating | 0.0 (0.0–2.0) | 0.0 (0.0–3.0) | 0.42 |
| Lower abdominal distension | 0.0 (0.0–2.0) | 0.0 (0.0–3.0) | 0.62 |
| Flatulence | 0.0 (0.0–2.0) | 0.0 (0.0–0.0) | 0.72 |
| Urgency | 0.0 (0.0–2.0) | 0.0 (0.0–0.0) | 0.68 |
| Incontinence | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.71 |
| Number of weekly evacuations | 7.0 (5.0–14.0) | 6.5 (0.0–9.0) | 0.08 |
| Bristol stool scale | 4.0 (3.0–5.0) | 4.0 (3.0–5.0) | 0.80 |
- Significant values are indicated in bold.

Box plots of upper and lower GI symptoms before (□) and during late COVID‐19 lockdown (■)
According to GAD‐7 questionnaire, 44 patients fulfilled the test and 17/44 (38.6%) showed the presence of anxiety.
According to PSS‐10 scale, it has been found perceived stress values ranging from 5 to 39 with an average and standard deviation (SD) of 17.9 ± 7.1. A significant correlation was found between anxiety and perceived stress levels (r = 0.66, p < 0.001).
Performing the logistic regression analysis higher anxiety level was the risk factor of worsening of chest pain, waterbrash, epigastric burning, and abdominal pain (Table 4).
Logistic regression analyses of higher anxiety level
| Symptom | OR | CI | p‐Value |
|---|---|---|---|
| Chest pain | 1.3 | 1.1–1.7 | 0.017 |
| Waterbrash | 1.3 | 1.0–1.7 | 0.024 |
| Epigastric burning | 1.3 | 1.0–1.6 | 0.043 |
| Abdominal pain | 1.6 | 1.0–2.3 | 0.015 |
When compared to the interval preceding the COVID‐19 outbreak, half of the patients declared that their FGIDs symptoms remained unchanged, 13.6% worsened or extremely worsened, whereas the remaining 36.4% improved or extremely improved. Figure 2 shows the percentage of patients who considered themselves improved, unchanged, and worsened compared to the interval preceding the COVID‐19 outbreak classified as Functional Heartburn (FH), FD, and IBS.

Percentage of patients who considered themselves improved, unchanged, and worsened compared to the interval preceding the COVID‐19 outbreak classified as functional heartburn (FH), functional dyspepsia (FD), and irritable bowel syndrome (IBS)
The multiple linear regression model with the answers to the online question: “Compared to the interval preceding the COVID‐19 outbreak, how would you score your symptoms?” (1 = extremely worsened; 2 = worsened; 3 = unchanged; 4 = improved; 5 = extremely improved) as dependent variable and perceived stress, anxiety level, age, sex, BMI, and FGID diagnosis as covariates demonstrated that the patient’s perception was significantly associated only with anxiety level (standardized B −0.52, p = 0.04).
4 DISCUSSION
In the present study, we investigated symptoms changes in FGID patients during the Italian lockdown due to SARS‐CoV‐2 pandemic and their relationship with levels of anxiety and perceived stress. Of note, we designed the study to enroll only FGID patients for whom a recent assessment of their symptoms was already available before the COVID‐19 lockdown. By designing the study in this way, we were able to have a baseline/reference time‐point against which to compare the intensity‐frequency scores of GI symptoms measured during the lockdown. To the best of our knowledge, this is the only study conducted in Italian patients with FGIDs during SARS‐CoV‐2 outbreak.
Our results demonstrated that despite COVID‐19 lockdown having forced an adaptation to home restrictions, the intensity‐frequency scores of several GI symptoms, improved between T0 and T1 and, especially, upper GI symptoms reached a statistical significance. As expected, the perceived stress was significantly correlated with anxiety level; however, only anxiety significantly influenced the worsening of several GI symptoms, in particular chest pain, waterbrash, epigastric burning, and abdominal pain.
The improvement of symptoms was in key with the patient’s answer to the question “Compared to the interval preceding the COVID‐19 outbreak, how would you score your symptoms?” that demonstrated only in 13.6% of patients an important worsening of symptoms compared to the interval before the COVID‐19 outbreak. Conversely, more than one third (36,4%) of our patients declared their FGID symptoms, improved or extremely improved. The patient’s perception of their FGID symptoms during COVID‐19 outbreak period was significantly associated only with anxiety.
Stressful life’s events causing worry, fear, and anxiety are able to activate the HPA axis, SAM and regulatory neuroendocrine systems, conditioning diseases onset and maintenance.3, 4 Several studies showed the psychological effects of forced quarantines on people during previous outbreaks. Hawryluck et al.1 showed how the 129 quarantined patients who answered a Web‐based survey exhibited a high prevalence of psychological distress during Toronto outbreaks due to 2002–2004 SARS pandemic. Jeong et al.2 reported that among 1656 patients who were in contact with MERS patients, 7.6% showed anxiety symptoms during the isolation period.
A recent work conducted by Mazza et al.28 on 2766 Italian people during COVID‐19 outbreak, based on online survey, showed that the acquaintance infection was associated with increased perceived stress levels, whereas a history of stressful situations was associated with higher depression and anxiety levels. Another Italian survey indicated that 38% of the general population perceived a form of psychological distress; however, the majority of subjects displayed no relevant distress.29
In this context, it is well known that brain and gut are closely related5 and anxiety disorders occur in 30%–50% of FGIDs’ patients. In a previous retrospective study, conducted on 4966 healthcare seekers, mood or anxiety disorders might be found more than 3 years before the FGIDs’ onset.30 Previous studies underlined how psychological stress and anxiety could modulate FGIDs and related symptoms severity, often in a negative way. Anxiety levels were shown to correlate negatively with gastric sensitivity in a FD subgroup considered hypersensitive to gastric distension.13 Another study that took into account both acute and chronic anxiety associated with impaired accommodation in FD confirmed previous pathophysiological studies in healthy volunteers showing an impairment of gastric accommodation during experimentally induced acute anxiety.13 In a recent study, focused on the relationship between co‐morbid FD and IBS patients and the severity of psychological symptoms, an independent association between anxiety levels and severity of GI symptoms was found after lactulose nutrient‐challenge test, in particular for symptoms as gas, bloating, nausea, and digestive comfort. These results confirmed that psychological states are important factors associated with FD symptom severity.31
In this study, the improvement, as at times modest, of intensity‐frequency scores of several of GI symptoms during lockdown reached the statistical significance. However, caution is required in the clinical interpretation of these results, especially when considering that these might be in apparent contrast with previous studies. This difference, indeed, might be explained by one or more of the following: focusing attention on an organic disease such as getting COVID‐19 might have lightened functional symptoms.32 Furthermore, the level of fear of getting COVID‐19 was lower in the studied population since it was from Campania, an Italian region that was affected by the pandemic much less than other northern regions. However, the percentage of anxiety in our FGID population (38.6%) is similar to the percentage demonstrated in another Italian survey performed in the general population (38%). In this last study, Authors hypothesized that the lack of anxiety in 62% of population was possibly due to the relatively short exposure to the pandemic, as well as to individual features promoting resilience. Confirming this hypothesis, another recent study conducted in the south of Italy demonstrated that patients with Multiple Sclerosis (MS), a chronic condition often coexisting with anxiety and depression, had no differences in their levels before and during lockdown. Authors suggested that these patients might be more accustomed to live with higher levels of anxiety compared to healthy people, showing a higher resilience to external events concerning all.33 Given that, the resilience might be considered one of the psychological aspects able to influence our patients’ symptoms improvement. A previous study demonstrated that lower resilience is associated with worse IBS symptom severity, lower IBS‐QOL, and stress hyperresponsiveness.34 Unfortunately, no studies have been performed on patients with other FGID. Other psychological factors might influence onset and maintenance of GI symptoms. In fact, for many functional patients copying and stress related to social activity and social interactions at work can be a more bothersome situation than being “closed” at home. Likewise, upper GI symptoms might have been positively influenced by eating at home a Mediterranean diet or, at least, having a more regular meals despite of having quick and qualitatively unhealthy meals at work. In addition, the psychological reactions to the lockdown are not a steady‐state status; in fact variations during the different phases of the lockdown have been described.35
However, in our patients’ higher anxiety levels rather than stress perception increased the risk of worsening chest pain, waterbrash, epigastric burning, and abdominal pain. These results are in key with previous findings that showed how anxiety is able to alter visceral pain stimuli brain processing and visceral motility patterns causing the symptoms worsening.10, 12, 13 This study has several limitations: our data are related to a single assessment of anxiety and perceived stress during COVID‐19 lockdown. Unfortunately, no stress or anxiety questionnaire was taken before the lockdown as well as after it. Moreover, we did not consider contingent situations such as divorces, job loss, and mourning that could impact stress perception, anxiety levels as well as resilience during lockdown period and, consequently, GI symptoms trend. Another limitation is the absence of a control group of healthy subjects; however, the strength of this study is to have a baseline/reference time‐point against which to compare the intensity‐frequency scores of GI symptoms measured during the lockdown. In addition, even if the assessments at both time points were completed with no assistance, modalities of administration differed slightly. At T0, patients completed questionnaires at our outpatients clinic, whereas at T1, completed questionnaires online at their own homes due to the Hospital rules of that period, which did not allow patient’s access for non‐urgent conditions. Lastly, the number of studied patients was low in comparison to the total number of FGID patients who were placed into quarantine and therefore it might impact the generalizability of our results.
5 CONCLUSIONS
In conclusion, an improvement of the majority of upper GI symptoms compared to before the COVID‐19 forced quarantine was found in our FGID patients. Although multiple psychological risk factors might be linked to GI symptoms onset and maintenance in FGID patients, in this study that investigated the impact of perceived stress and anxiety on GI symptoms, only anxiety was associated with a significant risk of worsening chest pain, waterbrash, epigastric burning, and abdominal pain.
DISCLOSURE
The authors have no conflicts of interest to disclose. This article is not submitted or under consideration by any other publication.
AUTHORS CONTRIBUTIONS
Giovanni Oliviero involved in study concept and design; analysis, interpretation and acquisition of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; literature research. Luigi Ruggiero involved in study concept and design; analysis, interpretation and acquisition of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; statistical analysis. Elvira D’Antonio involved in study concept and design; acquisition of data; critical revision of the manuscript for important intellectual content; literature research. Mario Gagliardi involved in study concept and design; acquisition of data; critical revision of the manuscript for important intellectual content; literature research. Rubino Nunziata involved in study concept and design; acquisition of data; critical revision of the manuscript for important intellectual content; literature research. Alessandro Di Sarno involved in study concept and design; acquisition of data; literature research. Carmelina Abbatiello involved in study concept and design; acquisition of data; literature research. Elvira Di Feo involved in study concept and design; acquisition of data; literature research. Simona De Vivo involved in study concept and design; acquisition of data; literature research. Antonella Santonicola involved in study concept and design; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; statistical analysis; literature research; study supervision. Paola Iovino involved in study concept and design; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; statistical analysis; literature research; study supervision.
REFERENCES

{kind=link}